
Since last year, the field of anaesthesia has been dominated by concerns arising from reports of serious neurological complications in children and adults of Venezuelan descent who have undergone general inhalation anaesthesia using halogenated anaesthetics. Hersill’s participation in the SEDAR (Spanish Society of Anaesthesiology, Resuscitation and Pain Management) National Congress on Paediatric Anaesthesia, held last November, provided an opportunity to address this issue and to connect with specialists working to shed light on it. Following these discussions with members of the working group of this scientific society, insights from various experts (three anaesthetists and a clinical pharmacologist) have been compiled, helping to provide a better understanding of the situation.
The first reported cases, from various countries including Chile, Colombia, Guyana, the USA, Germany and Spain, described neurological damage predominantly affecting the basal ganglia, resulting in severe impairment of motor function and, in some cases, death.
Initial evidence

Dr Pascual Sanabria, Head of the Paediatric Anaesthesia Department at La Paz Children’s Hospital in Madrid and a member of the ‘Mitochondrial Alert’ Working Group of the Spanish Society of Anaesthesiology (SEDAR)
As explained by Dr Pascual Sanabria, Head of the Paediatric Anaesthesia Department at La Paz Children’s Hospital in Madrid and a member of the ‘Mitochondrial Alert’ Working Group of the Spanish Society of Anaesthesiology (SEDAR), a possible pharmacogenetic association was considered in light of these events, that is, possible inherited genetic mutations (DNA) that could potentially influence the response to an anaesthetic agent or another specific medication.
Anesthetists from a number of countries, concerned by this finding, sent biological samples from patients who had suffered these neurological complications to the laboratory of Eduardo Ruiz Pesini, PhD in Biochemistry at the Aragon Health Research Institute and group leader at CIBERER at the University of Zaragoza. His areas of research include mitochondrial pathology and rare diseases caused by disorders of mitochondrial oxidative phosphorylation, as well as the pharmacogenetic effects of drugs, including anaesthetic agents such as volatile anaesthetic gases.
Their studies identified a possible association between a mitochondrial DNA variant (m.11232T>C) and severe neurological complications following exposure to general anaesthesia in paediatric patients. The research documents that the genetic variant could increase the sensitivity of cells to the inhalational anaesthetic sevoflurane, whilst no differential effects were observed with intravenously administered anaesthetics, such as propofol.>
As Dr Sanabria explains, cybrids—cell models that incorporate the mitochondria of the patient under study into a controlled environment—were used, enabling the assessment of their metabolism and pharmacological response. These ensayos mostraron una alteración significativa y dosis dependiente del metabolismo mitocondrial ante sevoflurano, no observada con propofol. El análisis genético posterior identificó en los pacientes afectados presentaban la variante m.11232T>C en el gen ND4, implicado en la cadena respiratoria mitocondrial, presente en situación de homoplasmia, lo que refuerza su posible papel patogénico en la respuesta adversa a anestésicos inhalatorios. “Esta mutación se ha descrito en individuos con ascendencia materna venezolana, especialmente con antecedentes familiares de la región de Carabobo (Venezuela), atribuyéndose el origen en población indígena de la región”, afirma.

trials revealed a significant, dose-dependent alteration in mitochondrial metabolism in response to sevoflurane, which was not observed with propofol. Subsequent genetic analysis identified that the affected patients carried the m.11232T>C variant in the ND4 gene, which is involved in the mitochondrial respiratory chain, present in a homoplasmic state, reinforcing its possible pathogenic role in the adverse response to inhalational anaesthetics. “This mutation has been described in individuals of Venezuelan maternal descent, particularly those with family origins in the Carabobo region (Venezuela), and its origin is attributed to the indigenous population of the region,” he states.
>
These findings have caused considerable concern due to the high volume of migration from Venezuela, driven by the country’s political and socio-economic situation; it is estimated that some eight million Venezuelans are scattered across the globe, with the largest concentrations in Latin America, the Caribbean, Brazil, the United States and Spain. The estimated number in Spain is around 650,000, with some 250,000 living in Madrid, followed by Catalonia, the Valencian Community and the Canary Islands, where the flow of migrants has not ceased.
The detection of three cases in Spain has led the SEDAR to set up a working group of anaesthetists to define strategies aimed at improving anaesthetic safety. These guidelines were issued in July 2025 as a “Health Alert” and were updated last April, with their publication in the Spanish Journal of Anaesthesia and Resuscitation. As Dr Sanabria describes, this is a protocol for at-risk populations — primarily people of Venezuelan maternal descent — which involves, in non-urgent procedures, carrying out a mitochondrial DNA genetic test to detect the mutation. This information makes it possible to estimate its prevalence, analyse the degree of mitochondrial impairment and advance pharmacogenetic studies, with the aim of identifying the safest anaesthetics and adapting the anaesthetic strategy to at-risk patients.
Spanish academic paper

Dr Elena Méndez, from the Maternity and Paediatric Anaesthesia Department at the Central Hospital of Asturias and a member of the SEDAR ‘Mitochondrial Alert’ working group.
The work and outreach carried out by SEDAR aim to provide professionals with knowledge and ensure patient safety. Thus, in addition to the alerts published by this scientific society and communications such as the one delivered during the National Congress of Paediatric Anaesthesia, a webinar was held in April, attended online by more than 250 professionals. During this event, clinical cases were presented, the mutation was described, ongoing pharmacogenetic research lines were outlined, and the need to report identified cases to promote pharmacovigilance was emphasised, in addition to disseminating and discussing the recommendations.
“At present, both children and adults of Venezuelan maternal descent are considered to be at risk, as the mutation identified in mitochondrial DNA is transmitted exclusively through the maternal line, and the cases described share this genetic variant, exposure to inhalational anaesthetics such as sevoflurane—which is more common in the paediatric population— with no adverse events observed with propofol, although the influence of other clinical or pharmacological factors cannot be ruled out,” states Dr Elena Mendez, of the Maternal and Paediatric Anaesthesia Department at the Central Hospital of Asturias and a member of the SEDAR ‘Mitochondrial Alert’ working group. .
In the cases described, the baseline neurological status was asymptomatic or stable, with no previous symptoms or abnormalities in tests that would have clearly identified the risk prior to surgery. As this specialist explains, no characteristic clinical profile has yet been defined, and the only factor that allows it to be detected is the presence of a mutation in mitochondrial DNA, in the ND4 gene (11232T>C). “This mutation can be identified through a laboratory genetic test, which is requested for at-risk groups, although it can delay the procedure by between 15 and 45 days. Its presence or absence helps anaesthetists choose the most appropriate anaesthetic techniques in each case,” she explains.>
In surgeries that cannot be postponed, such as emergency or cancer surgeries, it is not possible to wait for the genetic test results. In these cases, anaesthetic techniques are used that have been shown to be safe in the presence of this mutation, although this significantly limits the available options. This limitation is particularly relevant in paediatric surgery, where inhalational anaesthetics are frequently used because they allow anaesthesia to be induced without injections and with less stress for the child.
Continuous monitoring of brain activity during surgery using brain function monitors that record the electroencephalogram (EEG) is considered particularly valuable, as it enables the detection of unexpected changes in the patient’s response to anaesthesia. This information helps to adjust the dose or change the anaesthetic to improve safety. Furthermore, as Dr Elena Mendez explains, it is important to take a personal and family history, particularly if there have been cases of delayed recovery from anaesthesia, neurological problems or unexpected complications during previous procedures.
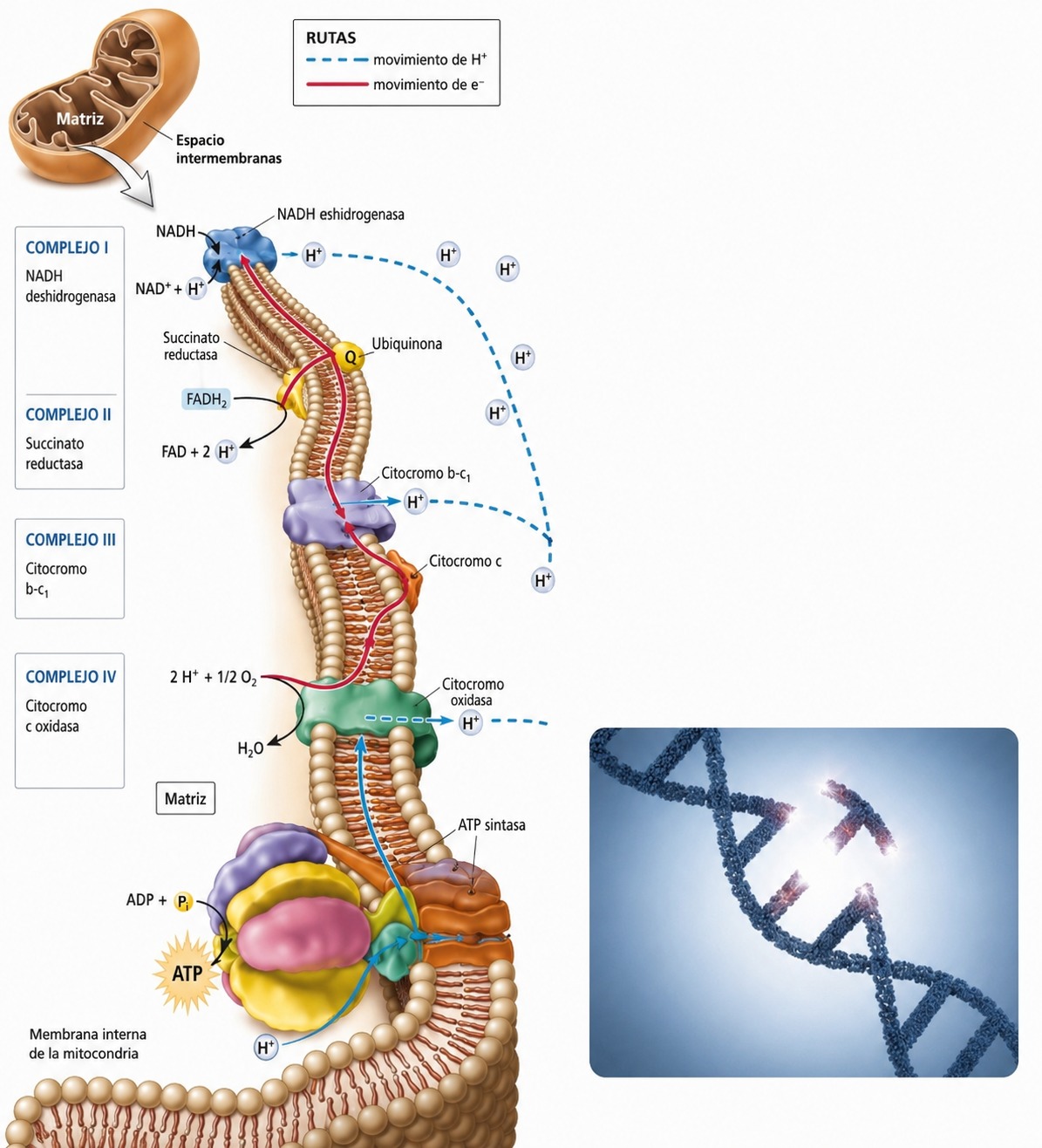
Electron transport chain. Mutations in mtDNA disrupt this system, leading to a critical shortage of cellular energy (ATP) when anaesthetic gases are used.
Current strategies
Dr Carlos Errando, Medical Director of Surgical Services at the Valencia University General Hospital Consortium and a member of the SEDAR ‘Mitochondrial Alert’ working group
According to Dr Carlos Errando, Medical Director of Surgical Services at the Consorcio Hospital General Universitario de Valencia and a member of SEDAR’s ‘Mitochondrial Alert’ working group,it is important to note that there are still some unknowns. On the one hand, from an epidemiological perspective, the frequency of these cases and their progression are not well understood, and terms such as “Venezuelan person” or “of Venezuelan mother” are not clearly defined. Nor is there conclusive data on who is most affected, whether children or adults. On the other hand, from a clinical perspective, there are still doubts regarding the role of prior exposure to anaesthesia, the possible under-reporting of cases, and the diversity of recommendations issued by different scientific societies.
“It is important to bear in mind that, in most reports, we are talking about individual cases, not even a series of cases. Furthermore, initial press reports contained incomplete or biased data, or raised doubts about the causal link between anaesthesia and death or severe neurological impairment in the perioperative period. Even the recommendations from scientific societies were, at first, relatively inconsistent, particularly regarding non-urgent procedures in children or the use of genetic testing, which is not available in most centres,” notes this expert.
In the patients described in greater detail, and particularly following the availability of genetic analyses suggesting a possible causal link—specifically, a susceptibility associated with the mtND4 m.11232T>C variant of complex I of the respiratory chain—the link with the use of sevoflurane as an anaesthetic agent appears clear.>
Dr Errando considers it important to note that sevoflurane is the most widely used inhalational anaesthetic agent in the paediatric population, both for deep sedation and for the induction and maintenance of general anaesthesia. This expert summarises the recommendations issued by SEDAR for patients of Venezuelan maternal descent who require surgical procedures or procedures under anaesthesia.
- As genetic testing is now available, SEDAR recommends postponing surgery in non-urgent cases so that the test can be carried out. In urgent or time-sensitive situations, the specific recommendations set out below apply.
- Following a pre-anaesthetic epidemiological screening, it is recommended that sevoflurane should not be used as an anaesthetic agent and, by extension, neither should any other halogenated anaesthetics (desflurane, isoflurane, halothane or others).
- Research is currently being conducted into the pharmacogenetic response of other drugs that could interfere with mitochondrial metabolic pathways.
- In urgent or time-sensitive cases, or where genetic testing has identified the mutation, local or regional anaesthesia is recommended, if possible. If this is not feasible, intravenous anaesthesia should be used. Any intravenous agent may be used; however, propofol (the most commonly used) is recommended at low doses and/or in infusions as limited as possible, due to the possibility that it may also affect the mitochondrial respiratory chain. To adjust the administration, it is recommended to monitor the depth of anaesthesia using processed EEG, avoiding periods of suppression, and to consider the use of controlled infusion techniques (CIT).
- It is recommended that the anaesthesia machine and circuits be flushed or cycled beforehand to remove any traces of halogenated anaesthetics.
- Strict monitoring of normoxia, normocapnia, normothermia and haemodynamic stability must be maintained, whilst avoiding hypotension and cerebral hypoperfusion. The use of near-infrared spectroscopy (NIRS) may be considered. Furthermore, metabolic monitoring of blood glucose levels and acid-base status is recommended.
- In outpatient surgery, the procedure may go ahead, but close post-operative monitoring is recommended until discharge, to ensure normal neurological recovery. The need for monitoring in high-dependency units is a matter of debate.
- In the event of abnormal awakening or the onset of neurological abnormalities in the postoperative period, an urgent neurological assessment is recommended, comprising both a clinical examination and imaging tests.
An overview of pharmacovigilance

Dr Elena Ramírez, from the Pharmacovigilance, Pharmacogenetics and Toxicology Unit at La Paz University Hospital, and director of the Patient Safety and Quality Research Group at IdiPAZ
Dr Elena Ramirez, from the Pharmacovigilance, Pharmacogenetics and Toxicology Unit at La Paz University Hospital and director of the Patient Safety and Quality Research Group at IdiPAZ, discusses the challenges posed by the mitochondrial genetic variant m.11232T>C> in her field.
In his own words, “to address the challenges and priorities surrounding the m.11232T>C variant in the mt-ND4 gene, it is essential to understand that we are facing a ‘double metabolic blow’ scenario; that is, a latent genetic vulnerability that manifests itself catastrophically in response to an external trigger, in this case, halogenated anaesthetics”.>
One of the main challenges for this expert is to determine the true scale of the problem, as bilateral striatal necrosis (BSN) is an extremely rare condition. In this regard, she considers it a priority to conduct studies to determine its incidence in the population of Venezuelan descent. Added to this is the need to correct potential misinterpretations in the genetic field, as this variant has historically been considered harmless, which may have led to underdiagnosis.
Another key aspect is the genetic complexity of the Venezuelan population, characterised by a high degree of racial mixing with Amerindian and African components, which are still under-represented in the scientific literature. Dr Ramirez believes it is essential to understand how these variants influence the body’s response to certain drugs in order to move towards more personalised medicine.
In emergency situations, where it is not always possible to rely on prior genetic testing, this also presents the challenge of identifying markers that enable the rapid detection of potential mitochondrial dysfunction during treatment. Furthermore, it highlights the need to develop therapeutic strategies aimed at improving the cells’ responsiveness, through treatments that optimise their energy metabolism or protect them from damage.
In this context, disciplines such as clinical genomics, pharmacogenetics and pharmacovigilance play a key role. Genomics allows for the more precise identification of the genetic variants involved, whilst pharmacogenetics helps to anticipate which patients may be more susceptible and to adapt treatments accordingly. For its part, pharmacovigilance is essential for detecting and recording new cases, issuing alerts and monitoring patients and their maternal relatives.
ongoing, the absolute clinical priority for patients of Venezuelan descent is to avoid sevoflurane, desflurane and isoflurane, opting instead for drugs considered safe, such as fentanyl, remifentanil, midazolam or dexmedetomidine,” she concludes.


